
On March 9, 2020, on a website promoting his health coaching and personal development business, Christian Elliot published a piece in which he stated "that the whole media frenzy about the Coronavirus is a bunch of money-making hype." One year and just under 3 million coronavirus deaths later, Elliot — a self-described "natural health nerd" who does not believe in germ theory — is back with more thoughts on the pandemic in a mega-viral article titled "18 Reasons I Won't Be Getting a Covid Vaccine."
Nearly all of the 18 reasons provided by Elliot are scientifically incorrect, overt misrepresentations, or irrelevant to the safety of COVID-19 vaccines. The post repeatedly pushes the false notion that COVID-19 vaccines do not prevent death, infection, and transmission. In several cases, Elliot misunderstands or misrepresents completely the data he cites to support his reasoning.
The ideas presented in the piece are not original, either. Virtually all of the claims in Elliot's article, when not years' old anti-vaccine tropes, can be tied to the most prominent anti-vaccine activists, contrarians, conspiracy theorists, or snake-oil salesmen of the COVID-19 era, including Sherri Tenpenny, Robert F. Kennedy Jr., Geert Vanden Bossche, Alex Berenson, and Joseph Mercola.
In this article, Snopes dissects, point by point, each of Elliot's "reasons" for not getting vaccinated against COVID-19.
#1 "Vaccine Makers Are Immune from Liability"
The first point on Elliot's list falls into the years' old anti-vaccine trope category.
It is true that vaccine manufacturers are shielded from liability. Without this liability protection, vaccine manufacturers were unwilling to supply the government with vaccines. As part of a 1986 compromise, the United States created legal protections for vaccine manufacturers while also establishing the National Vaccine Injury Compensation Program (VICP), a federal claims court that settles cases of alleged vaccine injury. As explained in Science, "The VICP was established after lawsuits against vaccine manufacturers and healthcare providers threatened to cause vaccine shortages and reduce vaccination rates."
While invoking this liability protection is a common anti-vaccine tactic, it is not a specific or novel argument unique to COVID-19 vaccines. All vaccines including the ones that have been required by schools for decades fall into this category.
#2 "The Checkered Past of the Vaccine Companies"
Pharmaceutical companies, including some involved in COVID-19 vaccine production, have indeed been fined billions of dollars in damages or criminal fines. Elliot asks "Given the free pass from liability, and the checkered past of these companies, why would we assume that all their vaccines are safe and made completely above board?"
Elliot's framing falsely suggests that the only check on vaccine safety derives from the word of the manufacturer. But all vaccines, including the COVID-19 vaccines, have all passed through phase I, phase II, and phase III trials, and these data are analyzed by both academics and government health officials. The process is not a rubber stamp of approval. The U.S. Food and Drug Administration (FDA) found problems in the way AstraZeneca presented its data to regulators, for example, and the agency has yet to approve the vaccine for use in the United States.
Elliot states that neither Moderna nor Johnson & Johnson had ever brought a vaccine to market before COVID-19. While true, neither company is inexperienced in vaccine development. Johnson & Johnson received long-awaited approval from the European Commission for a vaccine against Ebola in July 2020. Moderna has been at the forefront of developing the mRNA technology used in both its vaccine and the Pfizer vaccine. Moderna and the U.S. government had already entered into a licensing agreement for this technology before the global COVID-19 pandemic was declared.
Although off topic, Elliot asserts in this section of the post that the Johnson & Johnson vaccine "contains tissues from aborted fetal cells." This is false. As Snopes explained in March 2021, embryonic stem cells are used in the production of the vaccine, the shot itself contains no material derived from fetal cells.
#3 "The Ugly History of Attempts to Make Coronavirus Vaccines"
The first attempted scientific assertion about COVID-19 vaccines presented by Elliot at this point is where things really get off the rails. The purported "ugly history" of coronavirus vaccine research stems largely from a factually deficient telling of events pushed by anti-vaccine activist Sherri Tenpenny. Snopes debunked her claims in detail in March 2021.
About four months ago, Tenpenny began making the claim that COVID-19 vaccines would begin to wreak "havoc on the lungs" in "four to 14 months." Her argument relied on the studies of SARS and MERS vaccines later cited in Elliot's post. The rhetorical trick employed by Tenpenny, who charges hundreds of dollars for her "Mastering Vaccine Info Boot Camp" class, is to highlight older studies describing scientific challenges identified over the past decade of coronavirus vaccine development and ignore the studies that show how they overcome these challenges.
These challenges concerned two types of negative outcomes observed in some trials of previous SARS and MERS vaccine candidates that researchers feared could also happen in COVID-19 vaccines. The first was the possibility that the vaccine could actually increase the susceptibility of cells to be infected through a process known as vaccine induced enhancement, or antibody-dependent enhancement. The second was that exposure to COVID-19 following vaccination could send your immune system into overdrive and destroy the lungs — an injury termed immunopathology.
Subsequent study on coronavirus vaccine research — ignored by both Tenpenny and Elliot — led scientists to understand that this suite of reactions, broadly speaking, would occur in vaccines that failed to do two things: first, generate high levels of neutralizing antibodies (in the case of vaccine-enhanced disease) and, second, produce an immune response dominated by what are called Th-1 cells as opposed to Th-2 cells (in the case of immunopathology). For this reason, researchers knew at the very start of the pandemic to focus their efforts on technology that produced neutralizing antibodies and avoided the production of Th-2 cells. The mRNA vaccine technology provides the ability to generate such a response.
An October 2020 report in the New England Journal of Medicine reported that “The mRNA-1273 vaccine [i.e Moderna] induced [Th1] biased … responses and low or undetectable Th2 … responses.” As reported in Nature, data from the Pfizer/BioNTech vaccine indicate a “TH1-biased response.” These, along with the 192,282,781 doses administered in the United States alone, are quite literally the data necessary "to suggest they overcame that pesky problem of Vaccine Enhanced Disease."
It bears mentioning that the "cytokine storm" described by Elliot, in which overzealous pro-inflammatory immune cells attack healthy tissue, is a characteristic of a Th-2-biased response. SARS-CoV-2, the virus that causes COVID-19, itself produces a strong Th-2 response — severe cases of COVID-19 are often characterized by cytokine storms. A good way to head off such a response is to get a COVID-19 vaccine.
#4 "The 'Data Gaps' Submitted to the FDA by the Vaccine Makers"
Elliot focuses extensively on what the FDA identified as "data gaps" in the approval reports for the Pfizer and Moderna vaccines to suggest the vaccines do not prevent transmission or mortality of COVID-19. However, these reports, published in December 2020, contain no data collected after November 2020. Writing in April 2021, Elliot ignores the data that includes the hundreds of millions of doses of COVID-19 vaccine that have since been administered. These data are providing more definitive answers to those questions. As described in an April 2021 feature in The Atlantic:
The vaccines from Pfizer-BioNTech, Moderna, and Johnson & Johnson seem to provide stronger and more lasting protection against SARS-CoV-2 and its variants than natural infection. They are excellent at reducing symptomatic infection. Even better, they are extraordinarily successful at preventing severe illness from COVID-19.
Countries that have vaccinated large percentages of their population quickly, such as the U.S., the United Kingdom, and Israel, have all seen sharp and sustained declines in hospitalizations among the elderly. Meanwhile, countries that have lagged in the vaccination effort—including the U.K.’s neighbors France and Italy, and Israel’s neighbor Jordan—have struggled to contain the virus.
#5: "No Access to the Raw Data from the Trials"
While the "raw data" from clinical trials is not widely available, data from the clinical trials referenced by Elliot along with their entire experimental protocols can be found in these two journal publications. Further, as described in the medical journal BMJ, "around 400 pages of summary data are available in the form of multiple reports presented by and to the FDA prior to the agency’s emergency authorization of each company’s mRNA vaccine."
Regardless, Elliot primarily uses this section of his post as a platform to grossly misinterpret how COVID-19 trials are conducted. Citing a BMJ editorial, Elliot noted that, in a Pfizer trial, "3,410 total cases of suspected, but unconfirmed covid-19 in the overall study population, 1,594 occurred in the vaccine group vs. 1,816 in the placebo group.” Elliot falsely interprets this statement to mean that some people in the trial were not actually tested for COVID-19:
Did they fail to do science in their scientific study by not verifying a major variable?
Could they not test those "suspected but unconfirmed" cases to find out if they had covid? Apparently not.
Why not test all 3,410 participants for the sake of accuracy?
The answer to these three questions, respectively, is "no," "they did," and "they did."
The faulty interpretation of data repeated by Elliot was popularized by Alex Berenson — described in The Atlantic as "The Pandemic’s Wrongest Man." As Kawsar Talaat, an assistant professor at Johns Hopkins University, explained in that story:
"Suspected but unconfirmed" refers to "people who call in and say, 'I have a runny nose.' So we mark them as ‘suspected.’ Then we ask them to take a PCR test, and we test their swab, and if the test comes back negative, the FDA says it’s "unconfirmed."
#6: "No Long-Term Safety Testing"
It is necessarily true that the world lacks long-term data on vaccines that are less than a year old. We also lack long-term data on the disease for which the vaccines are designed to stop, but what little data we do have suggests the possibility of long and lasting effects in severe cases of COVID-19. Elliot implores his readers to wait until "those pesky data gaps" have been filled, but as described above, many of those gaps are already filled at this point.
#7: "No Informed Consent"
Contrary to the assertions made in this blog post, COVID-19 vaccines that have been granted emergency use authorization in the U.S. have completed phase three trials — or at least an interim analysis of a phase three trial — before being approved. It is not true, as claimed in the post, that any person given a COVID-19 vaccine is part of a clinical trial.
Elliot implies that the FDA is hiding, or would hide, the harmful effects of vaccines from the public. "If the vaccines are causing harm," he opined, "wouldn't we be seeing that all over the news? Surely the FDA would step in and pause the distribution?" At the time of this reporting, the biggest news in the COVID-19 vaccine space is that the FDA paused the distribution of the Johnson & Johnson vaccine in response to six blood clotting cases out of nearly 7 million doses administered.
#8: "Under-Reporting of Adverse Reactions and Death"
This point — the claim that adverse reactions to vaccines are under-reported — is another example of a years' old anti-vaccine trope. Here, the assertion is repurposed to imply that the number of adverse reactions to COVID-19 vaccines reported to the National Vaccine Adverse Events Reports System (VAERS), a federally run program designed to monitor vaccine safety, is likely massively undercounted.
Elliot asserts that these reports show that there have been "over 2,200 deaths from the current COVID vaccines, as well as close to 60,000 adverse reactions." VAERS is a self-reported system that in no way determines the cause of death or association with a vaccine. Just because someone died several months after they got a vaccine does not mean, as often claimed by activists, that a vaccine caused that death.
Using something purported to be a "Harvard study" (but that is actually a grant report on a project that could not be completed), Elliot performed some truly outrageous back-of-the-envelope math based on that report's claim that VAERS only captures 1% percent of total incidents:
If those numbers are still only 1% of the total adverse reactions ... you can do the math, but that equates to somewhere around 110,000 to 220,000 deaths from the vaccines to date, and a ridiculous number of adverse reactions.
With respect to the 1% figure, extrapolating it to cases of death rests on the false assumption that reporting rates for all adverse events, regardless of severity, are the same. As a spokesperson for the Centers for Disease Control and Prevention (CDC) told Reuters, reporting rates for different types of adverse events vary:
Mild events, like a rash, tend to be reported less frequently than severe events (like a seizure). We have data to show that serious adverse events that occur after vaccination are more likely to be reported than non-serious adverse events. Events such as a sore arm at the injection site might not get reported since they are expected and therefore people don’t feel the need to report them.
If your mathematical analysis leads you to claim that there have been 220,000 vaccine caused deaths that have somehow flown under the radar in a climate where six blood clotting incidents paused the distribution of a vaccine, it might make sense to challenge the assumptions that brought you to that "ridiculous number" in the first place.
#9: "The Vaccines Do Not Stop Transmission or Infection"
Elliot again repeats the false assertion that vaccines do not stop viral transmission or infection. The post asks "If we're worried about asymptomatic spreaders, would the vaccine not make it more likely that we are creating asymptomatic spread?" No, the empirical data on this point is clear: The vaccines reduce asymptomatic transmission. "If it indeed reduces symptoms, anyone who gets it might not even know they are sick and thus they are more likely to spread the virus, right?" Again, no, because the vaccine reduces asymptomatic spread and viral load.
#10: "People Are Catching COVID After Being Fully Vaccinated"
Some people have caught COVID-19 after being vaccinated. This is not unexpected. When vaccine manufacturers say their product is, for example, 95% effective, that means it will be not effective in 5% of cases. When you have administered over 100 million doses of vaccine, you are going to find cases of people for whom the vaccine did not prevent infection. Even in those cases, however, it is likely that the vaccine still helps to reduce the severity of infection.
#11: "The Overall Death Rate from COVID"
Elliot asserts that COVID-19 has a "99.74%" survival rate. It is unclear when or where Elliot got this figure, but it was almost certainly not the CDC, as claimed. Determining such a number is challenging for several reasons, and the number can change over time. At the time of this reporting, according to Johns Hopkins University, the case fatality rate for COVID-19 in the United States — the number of deaths per 100 confirmed cases — is 1.8%. As Anthony Fauci explained during congressional testimony, even a rate of 1% would make COVID-19 10 times more lethal than the seasonal flu.
#12: "The Bloated COVID Death Numbers"
COVID-19's death numbers are not "bloated." Once again, Elliot is making an argument rooted in a complete misunderstanding of the data he touts as evidence. In this case, the faulty logic has its origins in a viral claim made by a QAnon twitter account that was retweeted by President Donald Trump in November 2020:
According to the CDCs own numbers, (scroll down to the section "Comorbidities and other conditions") only 6% of the deaths being attributed to covid are instances where covid seems to be the only issue at hand.
In other words, reduce the death numbers you see on the news by 94% and you have what is likely the real numbers of deaths from just covid.
The CDC report Elliot references is a table that shows "Number of COVID-19 deaths with contributing conditions." The table is introduced with the explanation that "for 6% of these deaths, COVID-19 was the only cause mentioned in the death certificate." Elliot suggests that these are the only pure COVID-19 deaths because no other cause can be blamed. This is absurd.
The very conditions listed on this table are, in several cases, those that are commonly produced by COVID-19, including pneumonia, respiratory failure, respiratory arrest, and cardiac complications. It is simply a gross misuse of this data to suggest that people who are listed as dying of respiratory failure and COVID-19, for example, are not legitimate COVID-19 deaths. As explained in an October 2020 Scientific American article, the records included in that 6% are mostly likely the result of incomplete reports:
Those death certificates were incomplete because the certifiers gave only the underlying cause of death and not the full causal sequence that led to it, [Robert] Anderson, [chief mortality statistician at the CDC's National Center for Health Statistics] says. Even someone who does not have another health condition and dies from COVID-19 will also have comorbidities in the form of symptoms, such as respiratory failure, caused by the coronavirus. The idea that a death certificate with ailments listed in addition to COVID-19 means that the person did not really die from the virus is simply false.
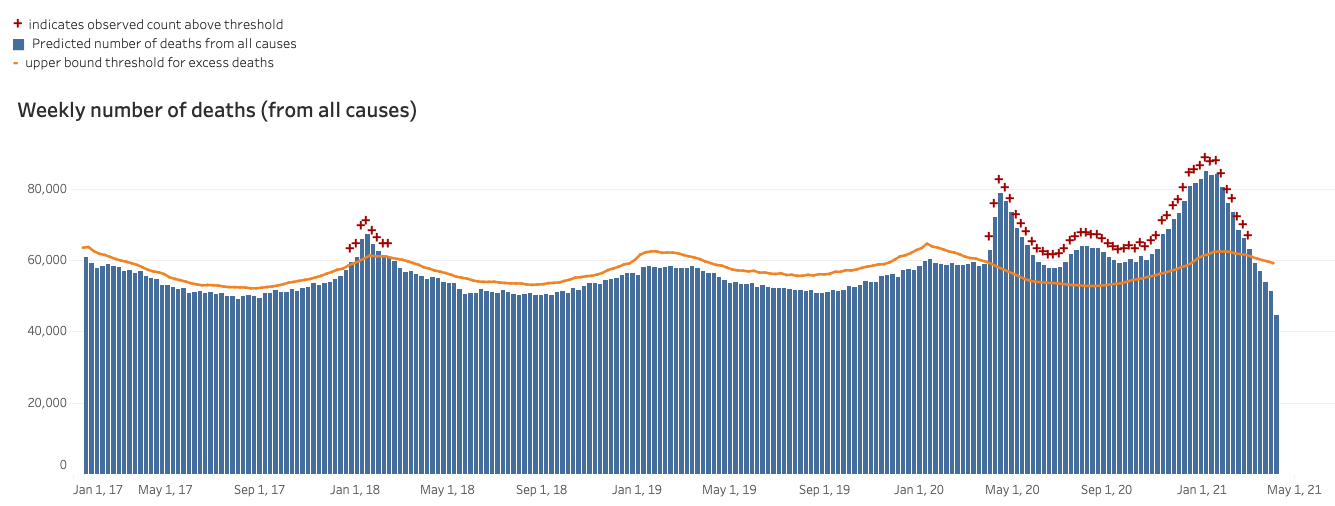
There are, as well, methods to calculate death tolls that are wholly unreliant on cause of death: one is a figure known as excess mortality. In simple terms, the figure compares the number of people expected to die during a given time period to the number of people who actually died during that time period. These data reveal that the U.S. is experiencing an unprecedented period of mortality that far exceeds the background level expected by the seasonal flu.
In the figure below, each bar represents the total number of deaths that occurred every week in the United States from January 2017 to the present, regardless of cause. The most recent weeks are undercounts due to the time it takes for the data to be reported. The yellow bar represents the expected number of deaths for that week. Any bar with a red cross at the top represents a week in which deaths were higher than would be expected:
#13: "Fauci and Six Others at NIAID Own Patents in the Moderna Vaccine"
This is not correct and it also isn't a critique of vaccine safety. It is, instead, an appeal to emotion that invokes the specter of Fauci, a boogeyman to the anti-vaccine/COVID-19 denial movement, to sow paranoia about ulterior motives.
The post asserts that "Tony Fauci owns over 1,000 patents … including patents being used on the Moderna vaccine." Elliot lifts this false notion from an interview between Naomi Wolf and Robert F. Kennedy Jr.. Kennedy, whose Instagram page spreading unhinged claims about 5G wireless technology, Bill Gates, and microchips, was banned in February 2021, is one of the most prolific spreaders of disinformation surrounding vaccine safety, and Ellliot cites Kennedy's Children's Defense Fund organization several times in his post.
Fauci is listed as an inventor on at least 36 patents or patent applications, according to a Google Patents search. Being an inventor does not mean that an individual "owns" the patent. These patents are owned primarily by the United States government or, in some cases, the academic institutions where most of the research was conducted. More to the point, however, Fauci himself does not own any patent related to any COVID-19 vaccine. The National Institutes of Health (NIH) does claim joint-ownership of the Moderna vaccine, and Fauci is director of the institute within the NIH that deals with vaccines. Prior to COVID-19 being declared a pandemic disease, in December 2019, the NIH had already signed a contract with Moderna to research coronavirus vaccines. As reported by Axios:
NIH and Moderna have researched coronaviruses, like MERS, for several years, and signed a contract this past December that stated "mRNA coronavirus vaccine candidates [are] developed and jointly owned" by the two parties. The contract was not specific to the novel coronavirus, and it was signed before the new virus had been sequenced.
Moderna had been, for years, developing the vaccine technology that allows for the delivery of mRNA to cells to produce custom-designed antibodies. When the pandemic struck, researchers at NIH sequenced, designed, and applied for a patent on the mRNA sequence that codes for the spike protein found in SARS-CoV-2. This genetic code is what is delivered by Moderna's technology.
As a result of that fact and the contract signed in December, NIH claims joint ownership of that vaccine. This is not done to enrich individual scientists in the U.S. government, but to allow for a "non-exclusive licensing approach for these patent rights in order to allow multiple vaccine developers" to produce COVID-19 vaccines. Both Pfizer and Johnson & Johnson use the NIH patented spike protein code as well.
The assertion that Fauci profits from the Moderna vaccine is false because Fauci doesn't "own" any relevant patent related to COVID-19 vaccine technology.
#14: "Fauci Is on the Hot Seat for Illegal Gain-Of-Function Research"
The post continues to veer off topic with more Fauci clickbait that heavily implies that the disease whose risks Elliot spent this whole post minimizing is also, maybe, actually, a genetically engineered supervirus:
What is "Gain-of-Function" research? It's where scientists attempt to make viruses gain functions--i.e. make them more transmissible and deadlier.
Sounds at least a touch unethical, right? How could that possibly be helpful? Our government agreed, and banned the practice.
So what did the Fauci-led NIAID do? They pivoted and outsourced the gain-of-function research (in coronaviruses no less) to China--to the tune of a $600K grant. Mr. Fauci, you have some explaining to do...and I hope the cameras are recording when you have to defend your actions.
The controversy over a $600K grant by the NIH to a New York Based non-profit EcoHealth Alliance that partners with the Wuhan Institute of Virology was popular early on in the pandemic, when people like Joseph Mercola — who has been fined millions of dollars over claims that tanning beds sold by his company would "slash your risk of cancer" — attempted to push the unsupported claim that COVID-19 was a bioweapon.
The $600K grant, which Fauci had no direct oversight over, was an extension of an existing grant that had been funded since 2014. The "illegal" gain of function research alleged to have been conducted through this grant was initiated before the U.S. imposed a pause on "Selected Gain-of-Function Research Involving Influenza, MERS and SARS Viruses." None of these conspiratorial diversions, however, hold any relevance to COVID-19 vaccine safety.
#15: "The Virus Continues to Mutate"
Earlier in his post, Elliot said he didn't trust Fauci because "he hasn't treated one covid patient" and because he allegedly had a financial interest in vaccine technology. It is odd, then, that his article places so much faith in Geert Vanden Bossche, a veterinarian who has spent the past decade trying and failing to patent something he calls a "universal vaccine" capable of killing a wide variety of diseases. His assertions, Snopes reported in March 2021, are part of a thinly veiled campaign to get people to pay more attention to an invention he tried and failed to patent at least twice.
In a series of viral posts published to his personal website in March 2020, Vanden Bossche argued that the current COVID-19 vaccines, through a mechanism analogous to antibiotic resistance, will create mutant variants of the virus that escape the protection of those vaccines. The only solution, he says, is his universal vaccine.
Viruses do mutate — this is not a surprise or a breaking news story. In places where his argument wasn't completely speculative, Vanden Bossche relied heavily on the notion that vaccines are unable to prevent asymptomatic transmission. This is an increasingly untenable position to argue, and pausing all vaccination, as Vanden Bossche advocates, will simply increase the rate and number of mutations occurring.
#16: "Censorship ... and the Complete Absence of Scientific Debate"
It is hard to take seriously allegations of "censorship" from someone whose blog post has been viewed over 2 million times and shared over a hundred thousand times on Facebook. There has been robust debate over myriad aspects of the pandemic including the reality of airborne transmission, the utility of lockdowns, how vaccine clinical trials are run, for example.
It is not censorship to point out that, for example, "suspected but unconfirmed" does not refer to people assumed to have COVID who have not been tested for it. It is not censorship to point out that claims of massive lung damage caused by vaccines stem from an argument from an activist who ignores all vaccine research conducted since the pandemic started. It is not censorship to point out that a back-of-the-envelope calculation asserting 220,000 vaccine-caused deaths relies on a series of massively untenable assumptions. And it is not censorship to report on the fact that COVID-19 causes death through the very same comorbidities that Elliot asserts are "bloating" the death toll.
#17: "The World's Leading Vaccinologist Is Sounding the Alarm…"
Vanden Bossche is not "the world's leading vaccinologist." As reported by McGill University's Office for Science and Society, "His academic publications essentially stop in 1995, except for one 2017 article about his … vaccine idea published in a journal belonging to a publishing group, OMICS Group Inc, that has been called “predatory” and was sued by the Federal Trade Commission for deceptive practices."
He does hold a Ph.D. in virology, and he has worked on vaccine development at several institutions. His ideas, as described above, are motivated by a belief that his invention, and his invention alone, can stop the pandemic, despite the fact that it does not exist. It is a speculative argument rejected by actual top vaccinologists.
The solution to that risk of COVID-19 variants is not to halt vaccination, as Vanden Bossche would like, but to vaccinate as many people as quickly as possible, thereby reducing both transmission of the virus and the number of environments in which mutations could occur. This is what COVID-19 vaccines do, and their widespread use serves to reduce the opportunities for the virus to mutate, and is why rapid vaccination is imperative.
“We’re in a race with the new variants,” Sara Del Valle, a computational epidemiologist at the Los Alamos National Laboratory in New Mexico, explained in a March 2021 feature in the scientific journal Nature. Waiting for Vanden Bossche’s “universal vaccine,” as we previously reported, is no way to win such a race.
#18: "I Already Had Covid"
Elliot asserts that he already had COVID-19 and that it wasn't all that bad. He claims that this means he has "beautiful, natural, life-long immunity" — an assertion based on eight months of data that does not speak to lifelong immunity. In other words, he is not going to get the vaccine because he, personally, survived unscathed and believes there remains no risk to himself.
But the vaccine hesitancy potentially inspired by these largely incorrect ideas increases the risk to everyone, including people not blessed, like Elliot, with an immune system capable of beating COVID-19. Vaccines are not only about protecting an individual, but about reducing the spread of a disease and environments in which viral mutations can occur.
The Bottom Line
The ultimate fallacy of this post is best expressed by a question posed by Elliot. "Why," he asked, "given that natural immunity has never ultimately failed humanity, do we suddenly not trust it?" Here's the thing — by asserting that natural immunity has "never ultimately failed humanity," Elliot appears to be setting the bar for a "real" public health emergency somewhere in the vicinity of the total extinction of our species.
Elliot is correct that humanity still exists despite several pandemics in the past. Such a framing of the problem betrays a truly breath-taking disregard for actual human life. The Plague of Justinian beginning in 165 A.D. killed an estimated 30 to 50 million people. The Black Death in the 1300s killed between 75 and 200 million people. When smallpox was introduced to the New World in the 1500s, some 25 to 55 million people were killed. The 1918 flu caused around 50 million deaths. Natural immunity quite literally failed these people.
Thanks to modern medicine, however, humanity is no longer forced to reckon with pandemic disease using only our "natural immunity." COVID-19 vaccines reduce death, infection, and transmission. Using a series of debunked falsehoods, Elliot argues that they don't and — further — that COVID-19 is not dangerous. As Saad Omer, an epidemiologist who serves as director of the Yale Institute for Global Health, told us earlier in a phone interview about claims made by Vanden Bossche, “The underlying fallacy is that a natural infection is better than a vaccine."